ELAPRASE® (idursulfase) was studied in a pivotal trial involving Hunter syndrome patients aged 5 years and older.
ELAPRASE was also studied in an open-label extension study and a safety study involving patients aged 7 years and younger.
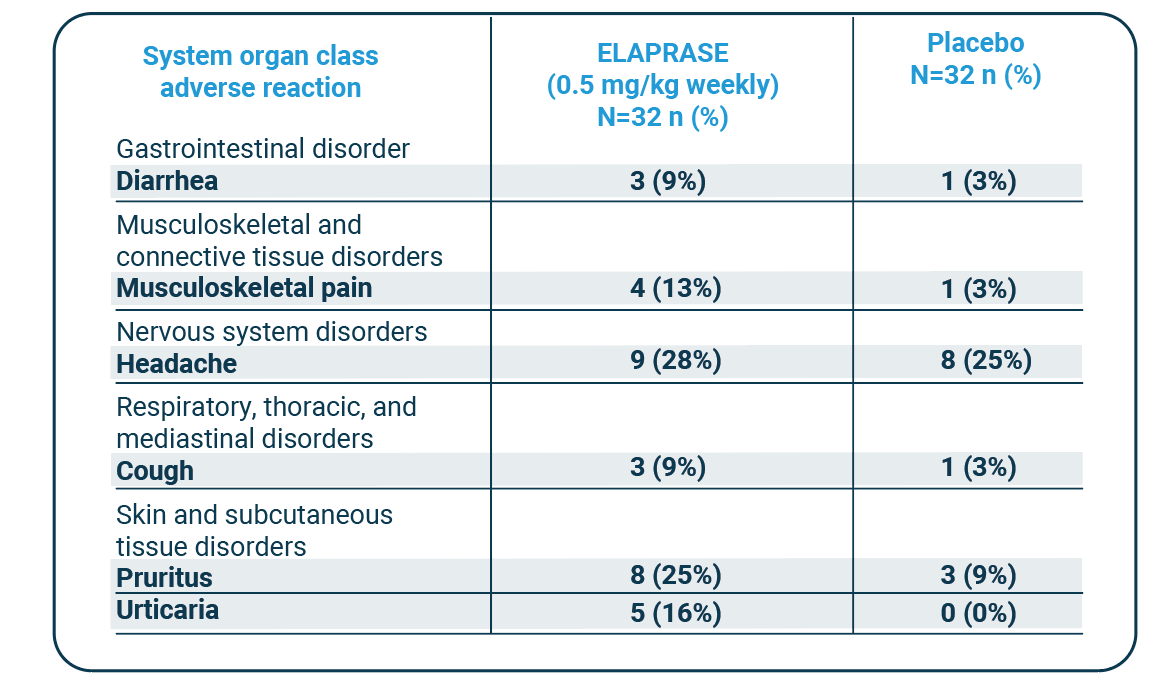
Adverse reactions (≥9%) occurring in the ELAPRASE group with a higher incidence than the placebo group (5 years and older)
| System organ class adverse reaction |
ELAPRASE (0.5 mg/kg weekly) N=32 n (%) |
Placebo N=32 n (%) |
|---|---|---|
| Gastrointestinal disorder | ||
| Diarrhea | 3 (9%) | 1 (3%) |
| Musculoskeletal and connective tissue disorders |
||
| Musculoskeletal pain | 4 (13%) | 1 (3%) |
| Nervous system disorders | ||
| Headache | 9 (28%) | 8 (25%) |
| Respiratory, thoracic, and mediastinal disorders |
||
| Cough | 3 (9%) | 1 (3%) |
| Skin and subcutaneous tissue disorders |
||
| Pruritus | 8 (25%) | 3 (9%) |
| Urticaria | 5 (16%) | 0 (0%) |
Extension trial safety profile
In addition to frequently experienced adverse reactions (see above) in the ELAPRASE once-weekly group in the pivotal trial (diarrhea [9%], musculoskeletal pain [13%], headache [28%], cough [9%], pruritus [25%], and urticaria [16%]), common hypersensitivity reactions occurring in at least five patients (≥5%) in the extension trial included:1
- Rash (23%)
- Pyrexia (9%)
- Flushing (7%)
- Erythema (7%)
- Nausea (5%)
- Dizziness (5%)
- Vomiting (5%)
- Hypotension (5%)
Under 7s safety profile
-
Patients aged 16 months to 7.5 years experienced similar adverse reactions to those observed in clinical trials in patients aged ≥5 years. The most common adverse reactions following ELAPRASE treatment were hypersensitivity
reactions (57%).1 -
A higher incidence of the following common hypersensitivity reactions was reported in this younger age group: pyrexia (36%), rash (32%), and vomiting (14%).1
-
The most common serious adverse reactions occuring in at least three patients (≥10%) included bronchopneumonia/pneumonia (18%), ear infection (11%), and pyrexia (11%).1
-
Patients with complete gene deletion or large gene rearrangement mutations are more likely to develop antibodies, including neutralizing antibodies, and to experience hypersensitivity reactions and serious adverse events, compared with patients with missense mutations with ELAPRASE administration.1
This table is intended as a summary only. In all clinical trials, the most common adverse reactions requiring medical intervention were hypersensitivity reactions, and included rash, urticaria, pruritus, flushing, pyrexia, and headache. Please refer to the Prescribing Information to read more about managing hypersensitivity reactions and see below for the full Important Safety Information including the Boxed Warning.
WARNING: RISK OF ANAPHYLAXIS
Life-threatening anaphylactic reactions have occurred in some patients during and up to 24 hours after ELAPRASE infusions. Anaphylaxis, presenting as respiratory distress, hypoxia, hypotension, urticaria and/or angioedema of throat or tongue have been reported to occur during and after ELAPRASE infusions, regardless of duration of the course of treatment. Closely observe patients during and after ELAPRASE administration and be prepared to manage anaphylaxis.